2022: Volume 4, Issue 2
Past Issues
 Abstract
Abstract  PDF
PDFAsymptomatic Isolated Congenital Cervical Dermal Sinus
Saeid Esmaeilian1*, Elham Mohajeri2, Behnam Kian1, Mehrdad Kayedi1, Mehdi Izadi1
1Radiologist, Department of Radiology, Shiraz University of Medical Sciences, Shiraz, Iran
2General Pediatrician, Shiraz University of Medical Sciences, Shiraz, Iran
*Corresponding author: Dr. Saeid Esmaeilian Department of Radiology, Shiraz University of Medical Sciences, Shiraz, Iran. Tel: 0910463698 E-mail: [email protected]
Citation: Esmaeilian S, et al. (2022). Asymptomatic Isolated Congenital Cervical Dermal sinus. Neuro Research. 4(2):12.
Received : May 22, 2022
Published : October 13, 2022
ABSTRACT
Introduction: Spinal Congenital Dermal sinuses are a rare condition which they are classified as an uncommon form of spinal dysraphism. Case Presentation: We had a rare case of cervical dermal sinus presented with non-tender midline cervical dimple without co-existing anomaly, who was referred for cosmetic reasons. MRI (Magnetic resonance imaging) showed a Dural sinus tract in the spinal canal of C2- 3, and a tract connecting it to the skin dimple. The spinal cord was thick and irregular with a small syrinx at this level. Also, spina bifida of C2-3 was noted. Conclusions: Dural sinus tract in the cervical area is a rare condition that presents with no symptoms in this case.
Keywords: Dermal sinus, cervical, spina bifida
INTRODUCTION
Spinal Congenital Dermal sinuses are rare conditions classified as an uncommon form of spinal dysraphism [1], embryologically that are supposed to be the consequence of failed neuroectodermal separation from cutaneous ectoderm during 3rd to 8th weeks of gestational age [2]. The most frequent site of occurrence has been described as the lumbosacral area and after that occipital region [3]. The cervical region is a very rare and uncommon site of occurrence [4]. Authors had been described other conditions that may be associated with a spinal dermal sinus that included fluid drainage from the spinal canal, epidermoid cyst or intradural dermoid [5], spinal cord tethering, teratoma [6] meningitis [7], and some neurological defect such as motor, sensory, gate and relaxes dysfunctions [8]. We report this very rare case describing an isolated cervical dermal sinus with no other complications.
CASE PRESENTATION
A 3-month-old girl had been referred due to an unusual posterior small deep hole in the midline of her upper neck at birth. The main reason for follow-up was the cosmetic condition. There was no history of discharge and no history of any infection such as meningitis or any developmental delay. No neurological problem was found in the family history. In the examination, a dermal orifice that had a small red halo was seen. No palpable mass was detected in the posterior part of the cervical area. A small amount of fluid with the pressure of the orifice was extracted. The patient’s vital sign was normal. No clinical or laboratory signs of infection were present.
Neurological Examination revealed a symmetrical movement of upper and lower extremities with No weakness. Deep tendon reflexes were Normal. Babinski’s reflex was present (normal at this age). No focal neurological deficit was found. Sonography examination showed “Oblique tract with diameter 2mm between skin dimple and spinal canal at cervical area.” CT scan (computed tomography) with 3D reconstruction revealed the defect of fusion of spinous process of C2–C3 (Fig. 1).
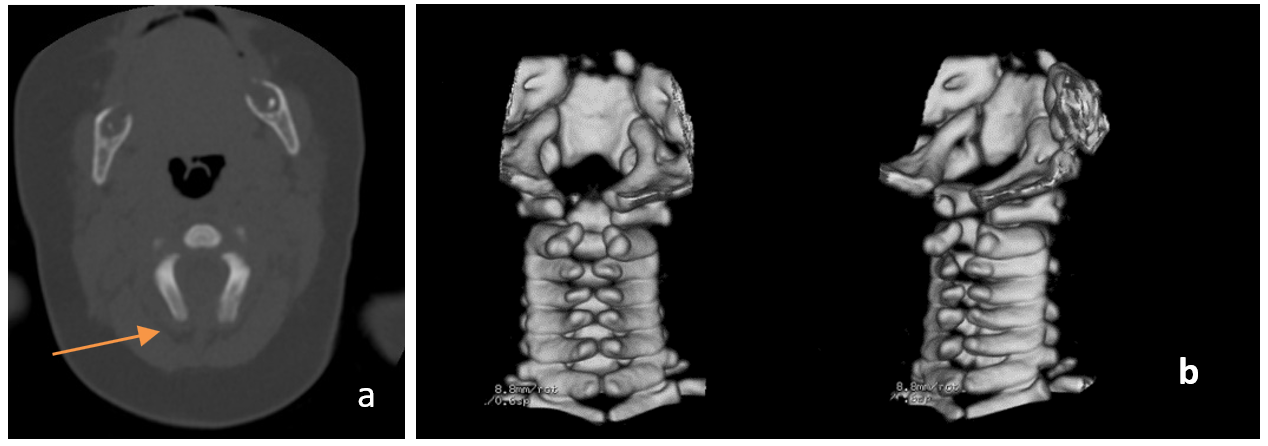
Figure 1: Spina bifida that present in the Axial cervical CT scan (a) with 3D images (b) C2-C3 level.
MRI shows the opening of the dermal sinus at the level of C2–C3 and the extension of the tract into the spinal canal associated with cord thickening and small syrinx (Fig. 2). On axial images, spina bifida at the level of C2-3 was noted. No Chiari malformation or other brain malformation was found. No other deformity in the rest of visualized part of the thoracic and lumbosacral area is noted.
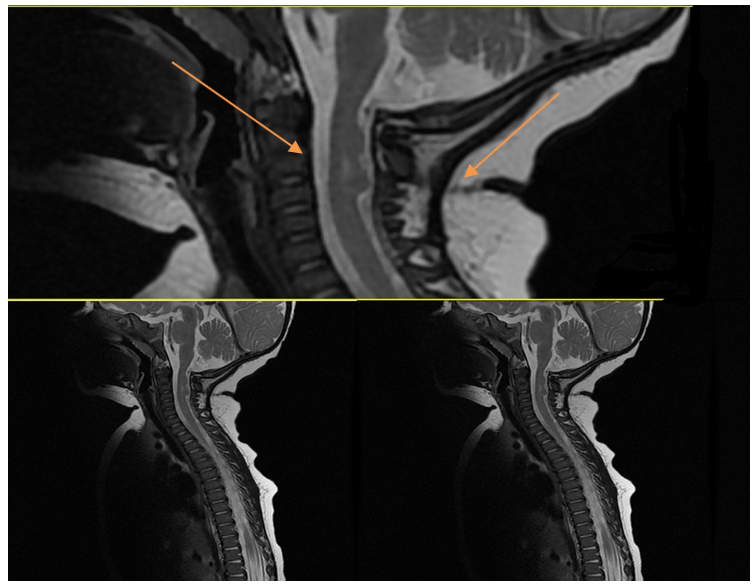
Figure 2: Sagittal T2-weighted MR image showing the opening of the dermal sinus at the level of C2–C3 and the extension of the tract into the spinal canal associated with cord thickening and small syrinx
Due to the risk of infection and accompanying neurological problems, surgical treatment should be performed as soon as possible. the sinus tract must be removed and the cord must be fully released. After a few days in the hospital, our patient underwent surgery. The tract was dissected down to the dura where the wall of the sinus was in continuity with the spinal dura. Samples were taken and sent for histopathological examination. histopathology revealed stratified squamous epithelium surrounded by dermal elements and fibro-fatty tissue. The bacterial culture was negative. Neurological examination after six months of surgery showed normal neurological development.
DISCUSSION
congenital spinal dermal sinus to be formed a Midline tract that is stratified by squamous epithelium n theory it is thought to result from the incomplete disjunction between the neuroectoderm of neural tube and the ectoderm layer of cutaneous [9,10].
Several adhesions layers can lead to the Extension of the tract and that may form from the deep fascia to the spinal cord. Elongation of the tract developed during the aging of the fetus, tract can rise from the cord and may be engaged to traverse several levels within the epidural space before entering the subarachnoid space. Another cause for forming the tract is Notochord Disorders which formed from sagittal splitting of the spinal cord and persistence of the dorsal cutaneous-endo-mesenchymal fistula [11, 12]. they can occur at any level though lumbosacral was the most common site after that occipital region [1].
Some case reports had described the cervical dermal sinus tract. Dubreuil published the first cervical dermal sinus in 1877 [5] after that other Authors had been described several cervical dermal tracts [2-4, 6-8, 10, 13] most of them had been associated with other neurological or non-neurological findings and in this case, our patient has isolated dermal tract sinus in comparison with other cases.
The point that made cervical reign a rare area for neurological dysraphism including the dermal sinus tract is that in the cervical region the neural tube fusion begins and then at the same time cranially and caudally it progressed to fusion and closing at the cephalad extremity. So dermal sinus has a high incidence in the areas that are closed by delay in comparison to other parts (specifically in the cervical area) [14].
Many cutaneous findings are described for associating with dermal sinus tracts including subcutaneous lipomas, flat capillary hemangiomas, hypertrichosis, pit, drainage of fluid or debris from the pit, and also an indirect sign of local infection [3] type of Infections that are described are included skin or soft tissue infection, meningitis or both. The infection process can lead to some complications such as hydrocephaly, although the incidence of this complication has not yet been determined in cases with congenital dermal sinus tracts [3] our described patient had none of these common features and conditions. Diagnosis is dependent on the type of symptoms that are present in the patient or even secondary complications. Since these lesions usually exceed the dura, screening for finding the lesions is not recommended except in suspicious patients. MRI is a choice modality for finding them, which provides important information on the neural structures and sinus tract relationship with other neural structures. In some cases, the sinus tract may not be well detectable on MR imaging if they are narrow or short. MRI will often reveal other consistent pathology such as intradural dermoid cysts. However, Diagnosis by MRI may be confusing in the consistent local infection or arachnoiditis, either of which can masquerade as an intradural lesion with clumping of the nerve roots. Ultrasound in these cases is more helpful. In addition, a CT scan with 3D reconstruction can lead to evaluating the bony part of the spine [3, 11, 15]. prophylactic surgical treatment of dermal sinus tract for prevention of infectious complications and tethered cord syndrome is recommended. our patient after a few days of hospitalization underwent surgery.no surgical complication was developed. neurological examination after 6 months was normal.
REFERENCES
1. Solak SS, Altunay IK, Demirci GT and Can B. (2016). Prevalence of congenital cutaneous anomalies in 1000 newborns and a review of the literature. Am J Perinatol. 33(1):79-83.
2. Sakr S, Mohan Y, Malik A, Malik G and Gonik B. (2015). Prenatal Diagnosis of Congenital Dermal Sinus. AJP Rep. 5(1): e43–e45
3. Elton S, Oakes W. (2001). Dermal sinus tracts of the spine. Neurosurg Focus. 10(1):1-4.
4. Shen WC, Chiou TL, Lin TY. (2000). Dermal sinus with dermoid cyst in the upper cervical spine: case note. Case Reports. 42(1):51-53.
5. Lee JK, Kim JH, Kim JS, Kim TS, Jung S, et al. (2001). Cervical dermal sinus associated with a dermoid cyst. Case Reports. 17(8):491-493.
6. Makary R, Wolfson D, Dasilva V, Mohammadi A, Shuja S. (2007). Intramedullary mature teratoma of the cervical spinal cord at C1–2 associated with occult spinal dysraphism in an adult: case report and review of the literature. J Neurosurg Spine. 6(6):579-584.
7. Bean JR, Walsh JW, Blacker MH. (1979). Cervical dermal sinus and intramedullary spinal cord abscess: case report. Neurosurgery. 5(1):60-62.
8. Ackerman LL and Menezes AH. (2003). Spinal congenital dermal sinuses: a 30-year experience. Pediatrics. 112 (3):641-647.
9. Ross M, Brewer K, Wright FV and Agur A. (2007). Closed neural tube defects: neurologic, orthopedic, and gait outcomes. Pediatr Phys Ther. 19(4):288-295.
10. Singh I, Rohilla S, Kumar P and Sharma S. (2015) Spinal dorsal dermal sinus tract: an experience of 21 cases. Surg Neurol Int. 6(Suppl 17): S429–S434.
11. McLone DG. (2001). Pediatric neurosurgery: surgery of the developing nervous system: Gulf Professional Publishing.
12. Pang D. (1992). Split cord malformation: Part II: Clinical syndrome. Neurosurgery. 31(3):481-500.
13. Radmanesh F, Nejat F and El Khashab M. (2010). Dermal sinus tract of the spine. Childs Nerv Syst. 26(3):349-357.
14. Morandi X, Mercier P, Fournier H-D, Brassier G. (1999). Dermal sinus and intramedullary spinal cord abscess report of two cases and review of the literature. Childs Nerv Syst.15(4):202-206.
15. O’Neill BR, Gallegos D, Herron A, Palmer C, Stence NV, et al. (2017). Use of magnetic resonance imaging to detect occult spinal dysraphism in infants. J Neurosurg Pediatr. 19(2):217-226.