2021: Volume 3, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFIsoMov-CG: A New Effective Therapy Programme Utilizing Isometric and Movement Exercises for Children with ADHD
Celestyna Grzywniak
Pedagogical University of Cracow, Poland
Corresponding Author: Celestyna Grzywniak, Pedagogical University of Cracow, Cracow, Poland, E-mail: [email protected]
Received Date: December 07, 2020 Publication Date: January 29, 2021
ABSTRACT
The article presents the results of a study conducted with early school children from Cracow who exhibited symptoms of ADHD. The experiment utilized a therapy programme by Celestyna Grzywniak which aimed at teaching the children to control their bodies, enhancing their concentration, reducing impulsiveness and encouraging them to follow the rules of a group.
The experiment lasted 9 months, the children attended classes twice a week. The programme utilized isometric and movement-based exercises, interviews with the children and their parents and learning to follow group rules. The article also presents ADHD in the classification of mental and behaviour disorders according to ICD-10.
KEYWORDS: ADHD; ADHD therapy; Therapy programme by Celestyna Grzywniak; Movement exercises
REVIEW
ADHD (Attention deficit hyperactivity disorder) is a set of symptoms in the range of hyperactivity, attention disorders and impulsiveness. According to ICD-10 (International Statistical Classification of Diseases and Related Health Problems), ADHD has three disorder areas: lack of attention, hyperactivity and impulsiveness. In this study, the interview intended for the teachers was composed on the basis of the symptoms presented in the ICD-10 classification, pages 139-141 (4).
The symptoms need to be present for at least 6 months causing inability to adapt presenting itself in various situations and places such as home, kindergarten, school or church. The symptoms need to appear before the age of 7 and must not meet the criteria of development disorders such as autism, the Asperger’s syndrome and others such as manic, depression or anxiety syndromes etc. According to DSM-5 (the American diagnostic criteria) the symptoms may appear later, even as late as at the age of 12.
According to ICD-10 (4), the first (I) area is the lack of attention –9 symptoms are enumerated and the child needs to exhibit at least six of them with significant severity which makes it impossible to function in a normal manner. The symptoms must be present for at least 6 months.
The symptoms are as follows:
The children:
- Do not pay close attention to detail or make careless mistakes in schoolwork or other activities,
- Often fail at focusing on tasks and activities involved in play,
- Often do not hear what is said to them,
- Often fail to follow instruction and do not finish schoolwork or homework,
- Often exhibit deficient ability to organize tasks and activities,
- Often avoid doing homework that requires mental effort or do it unwillingly,
- Often misplace things such as school aids, toys or other tools,
- Often have their attention dispersed due to external factors,
- Often forget things in the course of everyday activity.
The second (II) area is hyperactivity which includes six symptoms. The child must exhibit three of those six symptoms for at least six months to a degree leading to inadaptability or inconsistent with the development level of the child.
The children:
- Often anxiously move their hands and feet, jiggle at their desks or on their chairs,
- Often stand up during lessons, walk around the classroom or move in other situations when it is expected of them to keep a seated position,
- Are often excessively active or get involved in situations in an inappropriate manner.
- Are often excessively noisy while playing and lack calmness during rest,
- Exhibit hyperactivity in their behaviour which is unacceptable by social context and expectations.
The third (III) area is impulsiveness with three emphasized symptoms, at least one of which must be exhibited by the child to a significant degree for a period of at least six months.
The children:
- Often answer before the question is finished,
- Are often unable to wait in queue or wait for their turn in games or other group activities,
- Often interrupt and disturb others (e.g. interrupt conversations or games conducted by others),
- Often speak in an excessive manner not paying attention to the environment.
Application of the therapy programme for children with ADHD by Celestyna Grzywniak
I applied the therapy programme for children with ADHD by Celestyna Grzywniak in order to lower the severity of the discussed symptoms, to stimulate the development of children and to test its effectiveness. Due to the research goal set as such, I formulated the following research issues.
The main research question
Is it possible (and if so, that what extent) to lower the severity of the ADHD symptoms in children with psychomotor hyperactivity by using the therapy programme by Celestyna Grzywniak?
Specific research questions
- Has the therapy programme, in the parents’ opinion, lowered the severity of the ADHD symptoms, and if so, to what extent?
- Has the therapy programme, in the teachers’ opinion, lowered the severity of the ADHD symptoms, and if so, to what extent?
- Which of the areas (attention, hyperactivity and impulsiveness), in the parents’ and the teachers’ opinions, have exhibited improvement and which have not changed to a satisfactory extent?
A comparison of other therapy programmes utilized in treating ADHD and using physical activity
Researchers are showing increased interest in treating ADHD using various non-pharmaceutical methods because, as shown by statistics, the number children with this syndrome are increasing rapidly. Also, more research confirms the theory that physical activity may effectively support the development of cognitive functions in children with ADHD. It is also confirmed by my research presented below as well as by those conducted by Martin Miklas et al (2020) or Eduardo Esteban Bustamant et al (2016) and Alyx Taylor et al (2019) and also many other great researchers of this issue. Miklas and his team’s research involved introducing physical exercises for children with ADHD with an intensity of 60-80% of the children’s capacity. The exercises were conducted while watching a film. The obtained results indicated a beneficial change on a level of high statistical significance of 2 parameters out of 15 measured. Another experiment, conducted by Alex Taylor and his team involved introducing 40 minutes of physical activity of average and high intensity for 11 weeks for children with ADHD aged 10 to 11. After finishing the therapy, the data reported by the teachers indicated that the symptoms of ADHD exhibited by the children were significantly less intensive and the children had much fun while exercising together. Further interesting results of their experiments were obtained by Eduardo Bustamante along with his team who conducted a 10-week physical activity programme. The results obtained in the range of executive functions, attention, memory were moderate while clinical results noted a substantial improvement. The programme also showed that what the children found important was the adults’ attention and the interest of the people conducting the therapy. The children who participated in the experiment were from poor families living in urban areas. Worthnoting is also an analysis of 23 research results that can be found in an article by Manuel Valentini and Nicolas Tonio (2019). These experiments were related to the influence of Tai-Chi and various yoga systems on children with ADHD aged 5 to 18. The authors reached a conclusion that children with ADHD who perform physical activity experience an improvement of executive functions, motor skills, attention and concentration as well as social behaviour.
The description of the studied group
The group consisted of children aged 9 to 12 with diagnosed psychomotor hyperactivity (ADHD). The diagnosis was made by the psychologists from the Psychological and Pedagogical Counseling Centers in Cracow and in some cases by a school psychologist. The children attended 3rd and 4th grades of primary school. Their development was inconsistent, many of them had difficulty in reading and writing and a diagnosed risk of dyslexia. Several children experienced problems with calculations and emotional development. Some of the children exhibited aggressive behavior in the form of getting in fights with peers, spitting and pushing. 36 children started the therapy and seven of them dropped out during its course. The reason was lack of motivation and the parents’ lack of persistency concerning the children’s attendance. After a child had been absent 3 times in a row without a reasonable excuse, they were removed from the list of participants. The qualified children were divided into three age groups. A detailed description of the children qualified for the ADHD therapy programme by Celestyna Grzywniak is presented in the table below.
|
The number of children |
Group |
The number of children in the group |
Sex |
Age range |
Average age |
|
|
Girls |
Boys |
|||||
|
29 |
I |
9 |
1 |
8 |
9.0-9.8 |
9.5 |
|
II |
10 |
4 |
6 |
9.8-10.5 |
10.1 |
|
|
III |
10 |
4 |
6 |
10.6-11.6 |
10.9 |
|
|
Sum |
3 |
29 |
9 |
20 |
9.0-11.6 |
10.16 |
Table 1: The description of the children participating in the ADHD therapy programme by Celestyna Grzywniak according to sex and age.
The above table shows that the therapy programme was attended by 29 children in 3 groups, including 9 girls and 20 boys. The first group comprised of the youngest children of the 3rd grade, the remaining two – of the older children.
The organization and the course of the classes
The children were divided into 3 groups. The first group consisted of 3rd grade children, the second and the third – of 4th grade children. The therapy classes were conducted twice a week, lasted 60 minutes with the participation of two or three supporting members of staff, who were students from a Facilitation of children’s development study group from the Institute of Pre-School and Early School Educationat the Pedagogical University of Cracow. They studied pre-school, early school and social care pedagogy.
The therapy classes were conducted between September 2017 and June 2018 in the Comprehensive School Complex No 1, Aleje Kijowskie 5 in Cracow.
In order to qualify the children to the therapy group I conducted interviews with the parents and the teachers. The interviews had been composed by me on the basis of the symptoms indicated in the ICD-10 as well as my own knowledge. While meeting the children I conducted an uncategorized interview and observation. I also provided the parents with guidelines on how to proceed further with the child, particularly in case the symptoms became more severe. During the course of the therapy programme the parents were able to consult the child’s problems and discuss further actions. During the conversation I asked them to fill in an interview questionnaire. I repeated this action in June 2018. I qualified 36 children for the therapy group, however due to various reasons 29 children finished the therapy. The classes were conducted twice a week and lasted 60 minutes each. The children were divided into age groups. Each of the meetings I conducted was planned and went according to my own programme dedicated to children with symptoms of ADHD. The programme elements that follow were flexible and sometimes some of them were omitted for the benefit of others.
The therapy programme for children with ADHD by Celestyna Grzywniak consisted of the following exercises:
- The meeting started with all the participants sitting in a circle and each of them talked about everything that had happened since the last meeting. At the same time we talked about behaviour and problem solving, organizing the day, spending free time etc. If a need of an individual conversation with a child presented itself, it took place after the class with a member of the staff. At this stage, the children received support and guidelines concerning solutions to their problems. At this stage of the therapy, the children learn to wait for their turn, listen when another child is talking, search for an alternative solution to the problem presented by another child. They also learn empathy and control over their impulsiveness.
- The second part of the class involved physical and isometric exercises. Isometric exercises involve the whole body, particularly large muscle groups and focus on static muscle flexing without limb movement. The basic exercise involves pushing a part of the body against a solid object e.g. the floor in a lying position or gripping hands, bending arms at elbows and flexing muscles for a fixed period of time e.g. 5 or 8 seconds. After the muscle flexing comes, their relaxation and focusing on the feeling that comes from the muscles being flexed and then relaxed and the other way round. This way the children start to realize when their bodies are tense and when they are relaxed. Therefore the aim of the exercise is to teach the children to concentrate on the task as hand, to control their bodies and to feel them better.
- The physical exercises at this stage were aimed at channeling the excess energy, further learning to concentrate and to control oneself. The exercises involve sitting in a circle and rolling two balls simultaneously to each other. It may begin with rolling only one ball but two or three enforce better concentration and hasten the action. Then I introduced grappling at 50% strength to remain standing the longest, playing roosters, throwing balls at targets or goal while one of the children acts as a goalkeeper and then precise mimicking movements of animals, the “guess who” game and other activities. At this stage the children also learn to follow the rules of conducting the exercises, wait for their turn, cooperate with other children, vent excessive energy, accept other children, concentration and control over their bodies.
- Then I used board and other games e.g. “countries and cities”, tic-tac-toe, ludo, Rummikub etc. It aimed at learning to respect and follow the game rules, to lose, to control emotions, to plan and anticipate etc. depending on the game. While playing, various subjects and problems were discussed. While playing, the children were often able to establish contact with each other, talked, became friendlier and began to better understand themselves and other children, named their emotions they were feeling and learned to control them.
- Further into the programme, the children did group work in order to learn to work in pairs and in groups, to organize and also experienced joy resulting from a fulfilled task or a job well done. At this stage of the therapy the children learned to appreciate others, listen to others, and appreciate themselves and others for a good idea or fulfilling a task. Group activities involved making occasional decorations, group drawings, decorating the classroom or hall, making decorations with animals made of chestnuts or acorns etc.
- The therapy sessions finished with relaxation and saying good bye together in a circle and a collective shout.
THE APPLIED METHODS
The study involved an experiment with one experimental group. The children were chosen for the group purposefully since they had been diagnosed with ADHD in the Psychological and Pedagogical Counseling Centers in Cracow or by school psychologists. The study involved 3 stages: During the 1st stage, a pre-test, the parents and the teachers were interviewed. Also, uncategorized interviews and observation involving children were conducted. The interviews were composed on the basis of the symptoms indicated in the ICD-10 and the author’s own knowledge. A different interview was composed for the teachers and the parents with regard to the severity of the symptoms. The 2nd stage involves the introduction of the therapy programme for children with ADHD by Celestyna Grzywniak and the 3rd stage is a post-test which involves interviewing the parents and the teachers again as well as interviewing and observing the children.
The statistical calculations were conducted using arithmetic mean and difference of means, t-student test, DoF – the number of degrees of freedom, standard deviation and statistical significance while the statistical significance in the obtained results was denoted p<0,01 as highly statistical. In order to find the answer to the first and the second research question I conducted interviews with the parents and the teachers, uncategorized interviews with the children and then a statistical analysis of the obtained results. The data obtained during the interviews is presented in table 2 and table 3 below.
Below I am presenting my questionnaire for the interview I conducted with the parents and the teachers and the obtained data is presented in tables 2 and 3 below.
Interview questionnaire on the occurrence of ADHD in children at early-school age intended for teachers and parents created by Celestyna Grzywniak
Name of the examined child and their age…………………
The questionnaire contains sentences determining the occurrence of symptoms and their intensity.
0 – lack of symptoms, 1 –symptoms sometimes occur, 2 – symptoms often occur, 3 – symptoms always or almost always occur. Please read the sentences below carefully and mark the number which best characterizes a given behaviour.
1. The child fidgets around and is unable to remain in their place 0 1 2 3
2. While sitting, the child unnecessarily moves their arms, legs, lips, stands up 0 1 2 3
3. The child is excessively talkative 0 1 2 3
4. During a break the child runs around crazily 0 1 2 3
5. During plays involving movement, the child has difficulty following the rules 0 1 2 3
6. The hyperactivity is accompanied by mean and aggressive behavior 0 1 2 3
7. The child finds it difficult to focus on lessons and homework, especially on details 0 1 2 3
8. The child exhibits low attention span 0 1 2 3
9. The child is unable to listen for a longer period of time 0 1 2 3
10. The child does not finish started sentences and follows given instructions inaccurately 0 1 2 3
11. The child forgets about daily chores and doing homework 0 1 2 3
12. The child’s desk and schoolbag are messy 0 1 2 3
13. The child finds it difficult to organize their work 0 1 2 3
14. The child loses their belongings 0 1 2 3
15. The child wants to answer question before raising their hand and listening
to the rest of the question 0 1 2 3
16. The child often interrupts conversations or activities of other children 0 1 2 3
17. The child often shifts from negative to positive emotions and vice versa 0 1 2 3
18. The child often argues with other children and makes noise 0 1 2 3
19. The child often gets angry and moody 0 1 2 3
20. The child is not willing or avoids tasks requiring mental effort 0 1 2 3
21. The child is sensitive and emotionally experiences various situations 0 1 2 3
22. The abovementioned symptoms occur in various situations and places e.g. at home, at school, on a playground, during PE classes 0 1 2 3
|
Children |
Interview with the parents |
|||||
|
Attention |
Hyperactivity |
Impulsiveness |
||||
|
before (max.36) The symptoms’ degree of intensity |
after |
before (max. 20) The symptoms’ degree of intensity |
after |
before (max. 16) The symptoms’ degree of intensity |
after |
|
|
1 |
24 |
18 |
19 |
15 |
12 |
9 |
|
2 |
25 |
18 |
17 |
13 |
14 |
10 |
|
3 |
28 |
26 |
15 |
11 |
10 |
8 |
|
4 |
14 |
10 |
16 |
11 |
10 |
7 |
|
5 |
18 |
12 |
15 |
9 |
10 |
7 |
|
6 |
25 |
17 |
14 |
9 |
12 |
8 |
|
7 |
22 |
12 |
16 |
10 |
8 |
7 |
|
8 |
18 |
16 |
15 |
8 |
8 |
6 |
|
9 |
28 |
10 |
18 |
9 |
12 |
10 |
|
10 |
18 |
12 |
20 |
11 |
10 |
6 |
|
11 |
15 |
11 |
15 |
10 |
11 |
8 |
|
12 |
17 |
14 |
20 |
15 |
10 |
8 |
|
13 |
18 |
15 |
12 |
9 |
12 |
8 |
|
14 |
19 |
16 |
20 |
14 |
11 |
8 |
|
15 |
25 |
19 |
17 |
12 |
13 |
9 |
|
16 |
25 |
23 |
17 |
13 |
12 |
10 |
|
17 |
22 |
19 |
20 |
14 |
15 |
11 |
|
18 |
28 |
22 |
19 |
10 |
10 |
8 |
|
19 |
26 |
20 |
14 |
9 |
15 |
12 |
|
20 |
20 |
17 |
20 |
15 |
14 |
10 |
|
21 |
23 |
16 |
19 |
14 |
13 |
9 |
|
22 |
22 |
17 |
19 |
13 |
14 |
10 |
|
23 |
28 |
25 |
15 |
11 |
11 |
9 |
|
24 |
14 |
10 |
19 |
11 |
10 |
7 |
|
25 |
18 |
12 |
18 |
11 |
10 |
8 |
|
26 |
23 |
16 |
20 |
11 |
15 |
11 |
|
27 |
27 |
21 |
19 |
10 |
10 |
7 |
|
28 |
20 |
16 |
20 |
13 |
15 |
13 |
|
29 |
20 |
15 |
18 |
11 |
14 |
10 |
Table 2: The results obtained during the interviews with the parents before and after the introduction of the therapy programme for children with ADHD by Celestyna Grzywniak.
|
Children |
Interview with the teachers |
|||||
|
Attention |
Hyperactivity |
Impulsiveness |
||||
|
before (max. 21) The symptoms’ degree of intensity |
after |
before (max. 12) The symptoms’ degree of intensity |
after |
before (max. 21) The symptoms’ degree of intensity |
after |
|
|
21 |
17 |
12 |
9 |
20 |
18 |
|
|
2 |
18 |
15 |
12 |
9 |
18 |
15 |
|
3 |
21 |
16 |
11 |
8 |
19 |
17 |
|
4 |
18 |
10 |
10 |
8 |
13 |
11 |
|
5 |
17 |
10 |
10 |
6 |
12 |
10 |
|
6 |
21 |
18 |
9 |
5 |
15 |
10 |
|
7 |
20 |
16 |
12 |
8 |
14 |
12 |
|
8 |
16 |
15 |
11 |
7 |
15 |
12 |
|
9 |
21 |
16 |
12 |
8 |
20 |
17 |
|
10 |
15 |
12 |
12 |
8 |
18 |
13 |
|
11 |
15 |
12 |
9 |
7 |
14 |
14 |
|
12 |
17 |
14 |
12 |
8 |
15 |
12 |
|
13 |
19 |
15 |
8 |
5 |
16 |
12 |
|
14 |
15 |
9 |
12 |
9 |
18 |
15 |
|
15 |
18 |
17 |
8 |
7 |
17 |
15 |
|
16 |
17 |
15 |
11 |
6 |
16 |
15 |
|
17 |
15 |
12 |
12 |
7 |
18 |
15 |
|
18 |
20 |
13 |
10 |
5 |
17 |
10 |
|
19 |
21 |
17 |
12 |
9 |
18 |
13 |
|
20 |
15 |
12 |
12 |
8 |
17 |
12 |
|
21 |
14 |
10 |
12 |
7 |
16 |
13 |
|
22 |
16 |
11 |
12 |
8 |
20 |
17 |
|
23 |
20 |
15 |
8 |
7 |
19 |
14 |
|
24 |
16 |
13 |
11 |
7 |
18 |
13 |
|
25 |
17 |
13 |
11 |
7 |
17 |
13 |
|
26 |
20 |
17 |
11 |
7 |
18 |
14 |
|
27 |
18 |
13 |
10 |
6 |
19 |
16 |
|
28 |
19 |
16 |
12 |
7 |
18 |
13 |
|
29 |
20 |
17 |
10 |
7 |
17 |
17 |
Table 3: The results obtained during the interviews with the teachers before and after the introduction of the therapy programme for children with ADHD by Celestyna Grzywniak.
Then I calculated the average results obtained from the score (which showed the severity of the symptoms) used in the interviews with the teachers and the parents as well as standard deviation. The results are presented below.
|
The interviewees and the areas of exhibited symptoms before and after the therapy |
Arithmetic mean |
The number of children |
Standard deviation |
|
|
Pair 1 |
P_Att_B |
21,7241 |
29 |
4,34163 |
|
P_Att_A |
16,3793 |
29 |
4,37047 |
|
|
Pair 2 |
P_HA_B |
17,4483 |
29 |
2,30816 |
|
P_HA_A |
11,4483 |
29 |
2,06305 |
|
|
Pair 3 |
P_Imp_B |
11,7586 |
29 |
2,09856 |
|
P_Imp_A |
8,7586 |
29 |
1,72493 |
|
|
Pair 4 |
T_Att_B |
17,9310 |
29 |
2,26670 |
|
T_Att_A |
14,0000 |
29 |
2,56348 |
|
|
Pair 5 |
T_HA_B |
10,8276 |
29 |
1,36458 |
|
T_HA_A |
7,2414 |
29 |
1,15434 |
|
|
Pair 6 |
T_Imp_B |
16,9655 |
29 |
2,07851 |
|
T_Imp_A |
13,7241 |
29 |
2,25034 |
|
Table 4: A presentation of the statistical average acquired during the interviews with the parents and the teachers before and after the introduction of the therapy programme as well as the result of the standard deviation. Abbrevations: P – Parents, T – Teachers, Att – Attention, HA – Hyperactivity, Imp – Impulsiveness, B – Before, A - After.
The table above shows that the highest average value is present in the area of attention before the introduction of the programme in the opinion of both the parents and the teachers and therefore this area had been disturbed the most before the therapy. Hyperactivity was the second in terms of severity according to the parents and impulsiveness – according to the teachers. The highest standard deviation – deviation from the average – was present in the data concerning attention as evaluated by the parents before and after the therapy which indicated more extreme results and therefore children with more severe symptoms. The lowest standard deviation was present in the results concerning hyperactivity as evaluated by the teachers before and after the therapy. It may have indicated less severe symptoms exhibited at school than at home which might have been the result of a more strict discipline enforced at school and the children trying harder to control themselves. In order to better present the obtained data, it is presented on Diagrams 1 and 2.
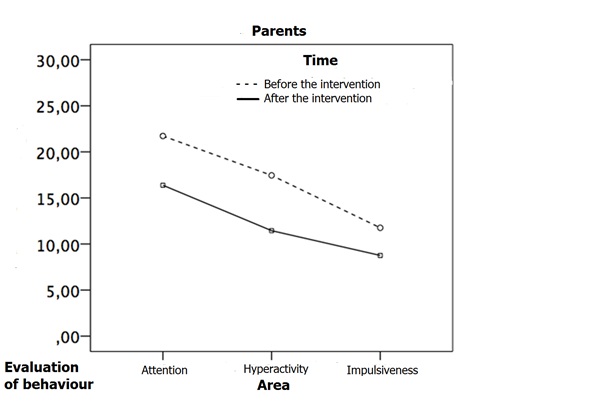
Figure 1: A comparison of the statistical average results obtained during the interviews with the parents conducted before and after the introduction of the therapy programme by Celestyna Grzywniak.
The diagram above presents the results obtained during the interviews with the parents conducted before and after the introduction of the therapy programme in three areas: attention, hyperactivity and impulsiveness. It clearly shows a decrease in the results in the second testing and therefore a decrease in severity of the ADHD symptoms. Similar data acquired during the interviews with the teachers is presented on Diagram 2 below. The teachers, as well as the parents, positively evaluated the influence of the therapy programme on lowering the severity of the ADHD symptoms in the children in question. It is indicated by the results obtained during the interviews conducted after the introduction of the therapy programme.
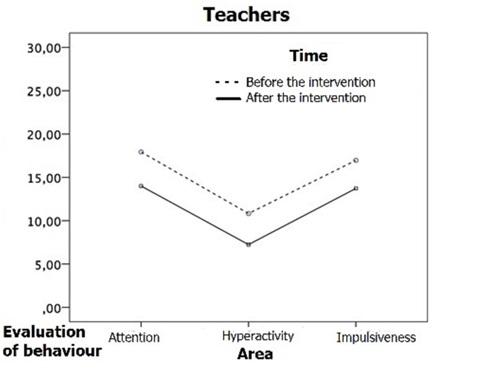
Figure 2: A comparison of the statistical average results obtained during the interviews with the teachers conducted before and after the introduction of the therapy programme by Celestyna Grzywniak.
The diagram shows a significantly lower severity of the symptoms in the three areas in the post-test.
Then I calculated the difference in the average values obtained during the interviews and the t-student test level as well as the statistical significance. The data is presented in Table 5.
|
The interviewees and the areas of exhibited symptoms before and after the therapy |
The differences in arithmetic means from the first and second test |
The t-Student test |
DoF – the number of degrees of freedom |
p –statistical significance |
|
|
Pair 1 |
P_Att_B P_Att_A |
5,34483 |
9,192 |
28 |
0,001 |
|
Pair 2 |
P_HA_B - P_HA_A |
6,00000 |
18,022 |
28 |
0,001 |
|
Pair 3 |
P_Imp_B - P_Imp_A |
3,00000 |
17,450 |
28 |
0,001 |
|
Pair 4 |
T_Att_B– T_Att_A |
3,93103 |
12,861 |
28 |
0,001 |
|
Pair 5 |
T_HA_B - T_HA_A |
3,58621 |
17,780 |
28 |
0,001 |
|
Pair 6 |
T_Imp_B - T_Imp_A |
3,24138 |
10,788 |
28 |
0,001 |
Table 5: A presentation of the difference in the average values obtained during the interviews with the parents and the teachers before and after the introduction of the therapy programme by Celestyna Grzywniak, the results of the t-student test, the numbers of the degrees of freedom as well as the level of the statistical significance.
Legend:
- Pair 1 and subsequent – the groups compared with each other using the t-student test, e.g. pair 1 is a comparison of the parents’ evaluation of the children’s attention before and after the introduction of the therapy programme.
- Abbreviations: P – Parents, T-Teachers, Att – Attention, HA – Hyperactivity, Imp – Impulsiveness, B- The result obtained before the introduction of the programme, A – The result obtained after the introduction of the programme
- Average – values of arithmetic means calculated for individual groups, e.g. the parents evaluating attention before the introduction of the programme, e.g. 21,724
- T-test – the t-student test
- DoF – the number of degrees of freedom
- P – statistical significance
The data presented in the table above indicates that the largest difference in arithmetic means was obtained in the area of hyperactivity (6,000) evaluated by the parents. It indicates that the children experienced the highest improvement and therefore it may be concluded that hyperactivity had been lowered the most after the introduction of the therapy programme. Another area in which a significant decrease of the severity of the symptoms had been achieved is attention, also highly evaluated by the parents. It may be concluded that the children had achieved very good results in this area. The teachers also observed a significant improvement in the area of attention in the children participating in the therapy programme. The lowest difference in arithmetic means was present in the area of impulsiveness as evaluated by the parents. It may be concluded that the improvement was relatively small, yet on a level of a high statistical significance. The level of the statistical significance of the obtained results indicates a high effectiveness of the utilized therapy programme as it is on the level of 0,001 in every evaluated area: the ability to pay attention and concentration, lowering hyperactivity and impulsiveness.
SUMMARY
The data presented in the tables and diagrams above indicates that the parents and the teachers, during the interviews, very highly evaluated the progress of the therapy of the children in the areas of attention, hyperactivity and impulsiveness. The comparison of the results obtained before and after the introduction of the therapy programme indicates a high statistical significance p=0,001 in the areas of attention, hyperactivity and impulsiveness. Therefore, hopefully, it may be possible to lower the severity of the ADHD symptoms in children by using the therapy programme by Celestyna Grzywniak.
The stated research questions may be answered positively; the introduction of the therapy programme by Celestyna Grzywniak, according to the parents and the teachers , had lowered the severity of the ADHD symptoms to a significant extent, which is confirmed by the high statistical significance in every area: attention, concentration, hyperactivity and impulsiveness. Answering the third research question, according to the parents, the area with the highest improvement was attention. It results from the fact that the parents pay more attention to the improvement in the area of hyperactivity and calmness of the child at home, while the teachers consider the child focusing on the task at hand and concentrating during classes a priority. The differences in opinion are confirmed by the results acquired from statistical evaluation.
BIBLIOGRAPHY
- Grzywniak C. Dojrza?o?? neuropsychologiczna do szkolnego uczenia si?, Scriptum, Kraków, 2017.
- Klasyfikacja zaburze? psychicznych i zaburze? zachowania w ICD-10, Uniwersyteckie Wydawnictwo Medyczne „Vesalius”, Instytut Psychiatrii i Neurologii Kraków – Warszawa-2000.
- Kryteria Diagnostyczne z DSM-5, Edra Urban & Partner, Wroc?aw, 2015.
- ICD-11 Governance and Process for ICD Revision, https://www.who.int/classifications/docs/ICDRevisionGovernanceFramework_V.Jan18.pdf?ua=1. Accessed on: 10-01-2020.
- Rigoni M, Zanardi Blevins L, Rettew DC. (2020). Symptom Level Associations Between Attention-Deficit Hyperactivity Disorder and School Performance. https://doi.org/10.1177/0009922820924692
- Bustamante E, Davis L, Frazier S, Rusch D, Fogg L, et al. (2016). Randomized Controlled Trial of Exercise for ADHD and Disruptive Behavior Disorders, Medicine and Science in Sports and Exercise. 48(7):1397-1407. https://doi.org/10.1249/MSS.0000000000000891
- Miklós M, Komáromy D, Judit Futó, Judit Balázs. (2020). Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study. International Journal of Environmental Research Public Health. 17(11):4071. https:// doi: 10.3390/ijerph17114071.
- Taylor A, Novo D, Foreman D. (2019). An Exercise Program Designed for Children with Attention Deficit Hyperactivity Disorder for Use in School Physical Education: Feasibility and Utility. Healthcare (Basel). 7(3):02. doi: 10.3390/healthcare7030102.
- Valentini M, Nicolas Toniol N. (2019). The benefits of physical exercise in children with attention deficit hyperactivity disorder (ADHD). Formazione & Insegnamento XVII – 3 – 2019 Codice ISSN 2279-7505 (on line)© Pensa MultiMedia Editore Codice. doi: 10.7346/-fei-XVII-03-19_33.
Copyright: Grzywniak C. ©2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Grzywniak C. (2021). IsoMov-CG: A New Effective Therapy Programme Utilizing Isometric and Movement Exercises for Children with ADHD. Neuro Research. 3(1):07.