2025: Volume 7, Issue 1
Current Issue
 Abstract
Abstract  PDF
PDFFibromyalgia Treated with Transcranial Direct Current Stimulation (tDCS) and Physical Exercise
Milton CR Medeiros1,*, Milton Takeshi Medeiros2, Marilia Mancebo3
1Irmandade Santa Casa de Arapongas, Rua Calu, 155, Arapongas PR, Brazil
2,3Centro Universitário de Valença – UNIFAA, Rua sargento Vitor Hugo, 161, Valença RJ, Brazil
*Corresponding author: Milton CR Medeiros, Irmandade Santa Casa de Arapongas, Rua Calu, 155, Arapongas PR, Brazil, Tel: 43999728197, E-mail: [email protected]
Received Date: June 17, 2025
Publication Date: July 04, 2025
Citation: Medeiros MCR, et al. (2025). Fibromyalgia Treated with Transcranial Direct Current Stimulation (tDCS) and Physical Exercise. Neuro Research. 7(1):23.
Copyright: Medeiros MCR, et al. © (2025).
ABSTRACT
Fibromyalgia is a chronic condition, characterized by diffuse musculoskeletal pain and associated changes (anxiety disorder, sleep disorder, depression, cognitive impairment, and fatigue). It is more common in women. Treatment methods include physical activity, cognitive behavioral therapy, and medications. Neuromodulation, especially transcranial direct current stimulation (tDCS), has been shown to have a significant impact on pain relief of fibromyalgia patients in many studies. In our research Ten outpatients, all women, participated in the study. They used different medications for fibromyalgia (anticonvulsants, dual antidepressants, tricyclic antidepressants and muscle relaxants) alone or in different combinations. All had intense pain, with a visual analogue scale (VAS) of 8 or more. These women were sedentary or did very little physical activity (less than once a week). The medications were maintained, and they were randomized into two groups matched by age. In group 1, five patients, with a mean age of 44.4 years old, received tDCS 2 milliamps for 20 minutes from Monday to Friday, for four weeks, with the anodal pole in the left motor area (M1) and the supraorbital cathodal pole on the right, without practicing physical activity. In group 2, five patients, with a mean age of 43,2 years old, received the same tDCS stimulus, but with physical activity (walking) of 150 minutes per week divided into 3 times. The VAS was reassessed at the end of treatment. The patients, all with severe pain (average of 8.5 on the VAS), were evaluated before the start of tDCS and after 4 weeks. All patients completed the study. Patients in group 1 (tDCS without physical activity) had the following VAS values after 4 weeks: 4, 3, 4, 5, and 3. VAS average of 3.8. Therefore, there was a significant reduction in pain intensity just by applying tDCS. In group 2 (tDCS associated with physical activity), the results were even better, with VAS after 4 weeks of 1, 2, 2,1 and 2. VAS average of 1,6. The differences between group 1 and group 2 were statistically significant, with t (t student) of 4.91and p less than 0,01. There were no side effects. In this randomized sample, it was possible to observe significant pain relief in patients with fibromyalgia. Studies have shown that the anodal stimulus in the primary motor area should be the one of choice for the improvement of pain sensation. So, tDCS is a promising method for the treatment of fibromyalgia, mainly due to its safety, low cost, and good efficacy. Our study suggests that the association of physical activity with tDCS intensifies pain improvement, when compared to tDCS alone. Studies with a larger number of patients should be carried out for more robust conclusions.
Keywords: Fibromyalgia, Disorder, Anodal Stimulation, Depression
INTRODUTION
fibromyalgia is a chronic and heterogeneous condition, characterized by diffuse musculoskeletal pain and associated changes, such as anxiety disorder, sleep disorder, depression, cognitive impairment and fatigue [1]. Fibromyalgia is a frequent cause of pain and affects about 2.5 to 3% of the world's population. It predominates in women and is an impacting factor in the worsening of quality of life, causing physical, emotional and financial damage [2]. The pain associated with fibromyalgia often is described as a constant dull ache that has lasted for at least three months. To be considered widespread, the pain must occur on both sides of body and above and below the waist [3]. Other condictions often co-exist with fibromyalgia, such as irritable bowel syndrome, migraine and other types of headaches, intersticial cystitis or painful blader, postural tachycardia syndrome and temporomandibular joint disorders syndrome. While there is no cure for fibromyalgia, a variety of treatment is avaliable. Fibromyalgia treatment involves various methods, such as physical activity, cognitive behavioral therapy, and medications. Unfortunately, these approaches do not offer satisfactory results for most patients. Medications, for example, have low efficacy and significant risks of side effects. The most commonly used drugs are tricyclic antidepressants such as amitriptyline, dual antidepressants such as duloxetine, and antiepileptics such as gabapentin and pregabalin [4]. Although there is no clear understanding of the disease’s etiology, the consensus on its pathogenesis is dysfunction in the central processing of pain perception and control systems that result in a state of increased sensitization to pain and Other stimuli [5]. Neuromodulation, especially transcranial direct current stimulation (tDCS), has been shown to have a significant impact on pain relief and functional improvement of fibromyalgia patients in many studies [6]. The tDCS is a neuromodulation method based on cortical modulation, producing facilitating or inhibitory effects in several brain areas. Popularity of the technique has grown over the past decade, as exemplified in a PubMed search, returning 1,500 published articles containing the phrase “tDCS” between 2011 and 2015, in comparison to just 65 articles published between 2000 and 2005. The tDCS involves the emission of a weak electrical current, traditionally via the placement of two electrodes, one anodal that facilitates neuronal depolarization and another cathodal that hinders neuronal depolarization [7]. The tDCS may offer a new line of treatment for fibromyalgia [8]. Another important modality for treating fibromyalgia is physical activity. International treatment recommendations for fibromyalgia highlight the importance of physical activity combined with patient education [9]. In this research, we will demonstrate the results of tDCS alone and tDCS plus physical activity in the treatment of fibromyalgia.
MATERIALS AND METHODS
Ten outpatients, all women, with fibromyalgia, participated in the study. All signed the informed consent form after detailed explanations about the method. They used different medications for fibromyalgia (anticonvulsants, dual antidepressants, tricyclic antidepressants and muscle relaxants) alone or in different combinations. All had intense pain, with a visual analogue scale (VAS) of 8 or more. These women were sedentary or did very little physical activity (less than once a week). The medications were maintained, and they were randomized into two groups matched by age. In group 1, five patients, with a mean age of 44.4 years old, received tDCS two milliamps for 20 minutes from Monday to Friday, for four weeks, with the anodal pole in the left motor area (M1) and the supraorbital cathodal pole on the right, without practicing physical activity. In group 2, Five patients, with a mean age of 43,2 years old, received the same tDCS stimulus, but with physical activity (walking) of 150 minutes per week divided into 3 or more times. The VAS was reassessed after 4 weeks of treatment.
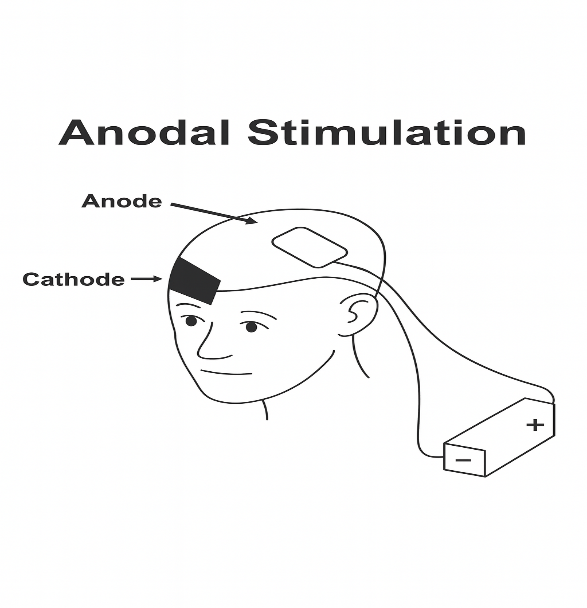
Figure A. Anodal stimulation in the primary motor cortex region on the left side and cathodal stimulation in the right supraorbital region. Fonte: ChatGPT.
RESULTS
The patients, all with severe pain before the procedure (average of 8.5 on the VAS), were evaluated before the start of tDCS and after 4 weeks, on the last day of tDCS. All patients completed the study. Patients in group 1 (tDCS without physical activity) had the following VAS values ??after 4 weeks: 4, 3, 4, 5, and 3. VAS average of 3.8. Therefore, there was a significant reduction in pain intensity just by applying tDCS. In group 2 (tDCS associated with physical activity), the results were even better, with VAS after 4 weeks of 1, 2, 2,1 and 2. VAS average of 1,6. The differences between group 1 (tDCS without physical activity) and group 2 (tDCS associated with physical activity) were statistically significant, with t (t student) of -4.91 and calculation of p showing very small number. There were no reports of significant side effects. In general, there were discrete paresthetic sensations of short duration at the site of electrical stimulation.
DISCUSSION
In this small randomized sample, it was possible to observe significant pain relief in patients with fibromyalgia. Studies have shown that the anodal stimulus in the primary motor area should be the one of choice for the improvement of pain sensations [10]. The procedure is cheap, safe and very well tolerated by patients, showing itself as a promising therapeutic technique for chronic pain in patients with fibromyalgia. In this study, the symptoms that accompany pain in fibromyalgia, such as sleep disturbances, fatigue, memory disorders, depression, or anxiety, were not evaluated. But, there are studies showing that pain is not the only symptom to improve in fibromyalgia, and there is an improvement in quality of life with the use of tDCS [6]. Regarding physical activity, several studies show its effectiveness for pain relief in fibromyalgia [9]. In our study, it was very evident that the association of tDCS with physical activity was much more effective than tDCS alone.
CONCLUSION
tDCS is a very promising method for the treatment of fibromyalgia, mainly due to its safety, low cost, and possible good efficacy Our study suggests that the association of physical activity with tDCS intensifies pain improvement, when compared to tDCS alone. Studies with a larger number of patients should be carried out for more robust conclusions.
ACKNOWLEDGEMENTS
None.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. (2010). The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken). 62(5):600-610.
- Freitas RPA, Andrade SC, Spyrides MHC, Micussi MTABC, Sousa MBC. (2017). Impacts of social support on symptoms in Brazilian women with fibromyalgia. Rev Bras Reumatol Engl Ed. 57(3):197-203.
- Abril A, Bruce BK. (2019). Mayo Clinic: guide for fibromyalgia.
- Gerardi MC, Batticciotto A, Talotta R, Di Franco M, Atzeni F, Sarzi-Puttini P. (2016). Novel pharmaceutical options for treating fibromyalgia. Expert Rev Clin Pharmacol. 9(4):559-565.
- Brighina F, Curatolo M, Cosentino G, De Tommaso M, Battaglia G, Sarzi-Puttini PC, et al. (2019). Brain Modulation by Electric Currents in Fibromyalgia: A Structured Review on Non-invasive Approach With Transcranial Electrical Stimulation. Front Hum Neurosci. 13:40.
- Fagerlund AJ, Hansen OA, Aslaksen PM. (2015). Transcranial direct current stimulation as a treatment for patients with fibromyalgia: a randomized controlled trial. Pain. 156(1):62-71.
- Thair H, Holloway AL, Newport R, Smith AD. (2017). Transcranial Direct Current Stimulation (tDCS): A Beginner's Guide for Design and Implementation. Front Neurosci. 11:641.
- Lloyd DM, Wittkopf PG, Arendsen LJ, Jones AKP. (2020). Is Transcranial Direct Current Stimulation (tDCS) Effective for the Treatment of Pain in Fibromyalgia? A Systematic Review and Meta-Analysis. J Pain. 21(11-12):1085-1100.
- Masquelier E, D'haeyere J. (2021). Physical activity in the treatment of fibromyalgia. Joint Bone Spine. 88(5):105202.
- Kang JH, Choi SE, Park DJ, Xu H, Lee JK, Lee SS. (2020). Effects of add-on transcranial direct current stimulation on pain in Korean patients with fibromyalgia. Sci Rep. 10(1):12114.